Empty Hours
What do the people of Albany Care do all day?

It’s the same building, more or less, though there have been big and small renovations over the years. Those years have also brought different names, different owners, different residents, different neighbors.
But some questions persist. Questions like this one:
The people who live at 901 Maple Avenue — how do they fill their days?
It’s a complicated question, without a single answer or answerer. The city of Evanston provides public spaces like Grey Park where Albany Care residents and neighbors can gather. Neighbors sweep and shovel the sidewalks, clearing the way for afternoon strolls. The business owners along Main Street know many of the Albany Care residents by name, greeting them and looking out for them.
Then there are the owners and operators of Albany Care. When a private company provides housing and psychiatric care for its so-called “consumers,” taking public funds to do so, what responsibility does that company have to help fill those hours? There’s the government, too. What duty does the state have to set standards for how that time is filled, and how well?
The SMHRF Administrative Code offers one answer:
Section 380.320 Recovery and Rehabilitation Supports Centers
f) Service Requirements
The recovery and rehabilitation supports center shall ensure that:
10) Consumers receive 15 hours of treatment programming per week, and that the care is documented in the consumer's medical record and is part of the consumer's treatment plan.
The precise language is important here. “Treatment programming” is therapeutic in nature, and includes such services as group and individual therapy sessions. (The requirement does not cover other types of activities, such as social events and recreational outings.) The language also specifies that SMHRF residents actually “receive” this programming. To meet the requirement, it’s not enough for the facility to simply offer it.
To be clear: SMHRF “consumers” have the right to refuse treatment, including medication and programming. But this doesn’t exempt the facility from making sure the requirement is met. If a SMHRF elects to admit a resident, they are assuming responsibility for ensuring the required care. This might mean adjusting group offerings to better meet the needs and interests of “consumers,” or using motivational interviewing techniques to help determine whether the people they admit are ready, willing and able to accept rehabilitative care.
So the requirement stands. How well does Albany Care meet it?
IDPH’s most recent annual survey of the facility, dated April 29th, 2025, cites nine areas of licensure violations. Category 5 of 9 relates to treatment programming. The surveyor first quotes the above language from the Administrative Code, then states:
This REQUIREMENT is not met as evidenced by:
Based on interview and record review the facility failed to ensure 15 hours of treatment programming for 9 (C1, C2. C3, C4, C5, C6, C7, C8 and C9) consumers of 9 consumers reviewed for 15 hours of programming as per regulations.
This has the potential to affect all consumers within the facility.
The surveyor goes on to list findings which support this conclusion, capping the section with an assignment of a LEVEL 2 violation for the reported failures.
The findings in the 4/29/25 survey do not reflect an isolated failure. A review of documents obtained through a FOIA request reveals other reported violations of the programming requirement, on surveys dated 4/1/24 (Annual Licensure Survey); 5/11/2023 (Annual Licensure Survey); and 10/5/22. The 10/5/22 survey documents several complaint investigations; the interviews in that survey appear to have been conducted during Albany Care’s 2022 period of Level 5 restricted licensure.
(These and other records contain evidence of additional violations, including numerous Level 3 violations, at least one Level 4 violation, and the Level 5 violation which preceded Albany Care’s current restricted license. Some of these violations will be the focus of future posts.)
What about other types of programming? Unlike treatment programming, SMHRFs are not required to provide regular actitivites or recreational offerings. But it stands to reason that such programming — things like art classes, field trips, game nights, job training programs — can help enrich the daily lives of the residents. They can offer space for connection among SMHRF residents, and with members of the shared Evanston community. And they can help prepare residents to achieve the goal inherent in the SMHRF name and model: transitioning to a healthy life outside the facility.
Documentation about Albany Care’s current activities isn’t readily available online. Though one could surmise, based on the consistent gatherings of residents in Grey Park, that structured recreational activities are inconsistent. (Of course, Albany Care residents have the right to safely enjoy the park and all public spaces; this is one of the benefits of placing a SMHRF in a residential neighorhood. The question is: do the residents have enough healthy, engaging alternatives beyond such defaults as sitting in the park, smoking, or watching TV?)
At one time, at least, it seems they did. Below is an excerpt from a 2012 newsletter published by Albany Care, and still available on the facility’s website.
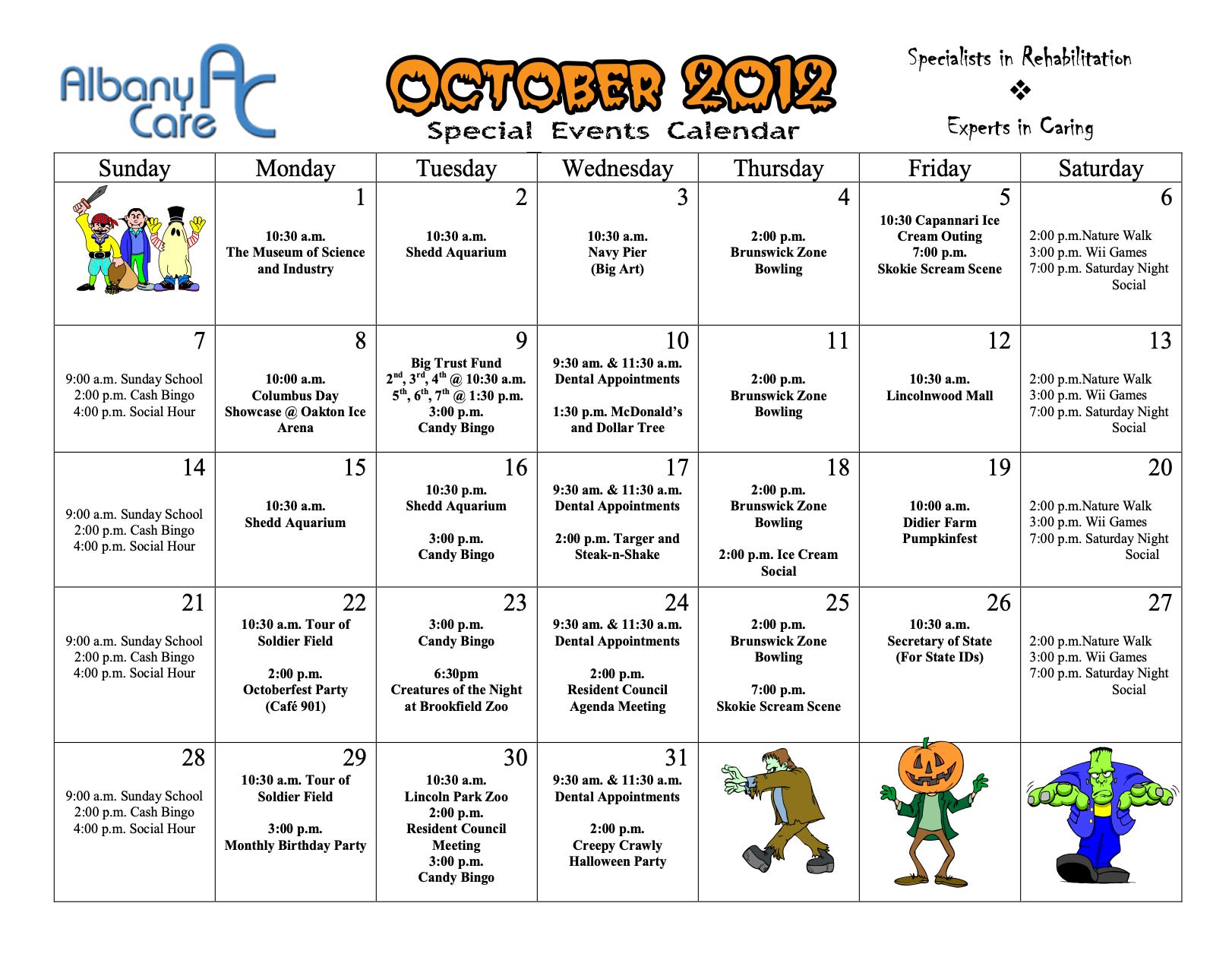
Albany Care maintains the same ownership and consultant entities it had in 2012. But the facility was not a SMHRF at that time; the SMHRF designation didn’t exist until 2013, and Albany Care didn’t transition to the SMHRF model until 2017. Also, while some employees from 2012 may still work at the facility today, different people fill key administrative and leadership roles. The ones who planned the slate from October 2012 aren’t there anymore, it seems.
Which leaves us with another question:
What should Albany Care do, and what more could it do, to help its residents fill the “empty hours?”